
© www.aafp.org
Viral infections are very common and readily transmitted through saliva and other body fluids. When there is close contact with other persons or their secretions and general hygiene is poor, viral infections mainly affect young children. However in developed countries, adults are non-immune and therefore, these infections are now being seen in adolescents and adults.
Infectious mononucleosis or glandular fever is caused by the Epstein-Barr virus (EBV), a member of the herpes group (human herpesvirus 4). It is transmitted by contact with saliva, especially by kissing, either from an infected person or a healthy carrier and occurs predominantly in teenagers and young adults.
What is infectious mononucleosis?

© Buzzle.com
Infectious mononucleosis syndrome is characterized by fever, lymph node enlargement and inflammation of the throat, and may be associated with prolonged periods of physical discomfort lasting months or more. Glandular fever is typically caused by Epstein-Barr virus, but also sometimes by other infectious agents for example human immunodeficiency virus (HIV) infection, cytomegalovirus infection, toxoplasmosis, infectious lymphocytosis and human herpesvirus 6 infection.
Epstein-Barr virus is found in saliva of the individual having infectious mononucleosis and for several months thereafter. The Epstein-Barr virus is often seen in saliva of persons who are unable to develop a normal immune response, which may cause hairy leukoplakia or lymphomas. Furthermore, Epstein-Barr virus may also cause sialadenitis, is associated with Burkitt’s lymphoma and has also been detected in mouth cancer.
Though infectivity is low, Epstein-Barr virus appears to be spread by close oral contact, such as kissing hence earning infectious mononucleosis the nickname ‘kissing disease’. Infection is common among young adults and is often subclinical or unrecognized, especially in children.
Infectious mononucleosis symptoms
Infectious mononucleosis causes mainly chronic abnormal enlargement of the lymph nodes, sore throat and fever but is variable in manifestations.
In children
- Generalised enlarged lymph nodes, typically with obvious enlargement in the neck region
- Sore throat
- Fever
In adolescents
- Enlarged lymph nodes that are often less obvious
- Vague illness with fever

Palatal petechiae © University of Birmingham UK
Palatal petechiae © University of Birmingham UK
In the anginose (Of or related to the pain of angina pectoris) type of disease
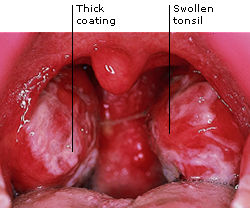
- Sore throat, oozing tonsils and swelling of the throat
- Palatal petechiae (A minute red or purple spot on the surface of the palate)
In the febrile (Of or relating to or characterized by fever) type of disease
- High fever
- Rashes that looks like rubella
- Occasionally jaundice.
In the glandular (Of or relating to the glands) type of disease
- Generalized lymph node enlargement especially the neck region
- Splenomegaly (abnormal enlargement of the spleen)
© All About Health
Within the mouth, the most typical manifestation of infectious mononucleosis is the merging creamy ooze in the passageway of the mouth, a spot of ruptured blood vessels at the junction of the soft and hard palate and inflammation. Ulceration in the mouth or gums may be seen, but the oral changes are non-specific.
Complications of infectious mononucleosis
Complications include:
- Persistent tiredness,
- Mild liver dysfunction,
- Electrocardiogram (ECG) changes,
- Depression,
- Neurological syndrome
- Rarely nephritis, pancreatitis or lung infiltration.
Management of infectious mononucleosis
The lymph node tissue changes in infectious mononucleosis closely resemble those in lymphomas (cancer of the lymph tissues) and an expert opinion is needed. A useful precaution in such cases is to have a blood examination and a test for heterophil antibodies.
Infectious mononucleosis diagnosis is confirmed by a peripheral blood picture showing the atypical (monocyte-like) lymphocytes. A heterophil antibody (Paul-Bunnell) infectious mononucleosis test and, if necessary, demonstration of a raised titre of Epstein-Barr virus antibodies are confirmatory. Heterophile antibodies are IgM antibodies that clump together sheep and horse red blood cells. The Paul-Bunnell test for infectious mononucleosis employs sheep red blood cells but more rapid methods are available to detect heterophile antibodies to horse red blood cells by detecting clumping on a glass slide (Monospot test). If these tests are negative in an otherwise typical case, cytomegalovirus infection or toxoplasmosis should be considered. Attainment of HIV infection frequently also gives rise to an illness resembling infectious mononucleosis.

This patient with infectious mononucleosis had been placed on ampicillin which resulted in a macular-papular skin rash. © Michael Finkelstein and Gilbert Lilly, University of Iowa College of Dentistry and Hardin MD, University of Iowa
There is no specific infectious mononucleosis treatment but infection is usually self-limiting but as there is frequently physical discomfort and tiredness, the individual may benefit from bed rest.
Ampicillin or amoxycillin should be avoided for they are prone to cause irritating macular rashes (discoloured patches of skin which are not usually elevated) unrelated to penicillin allergy, affecting mainly the limbs.
Systemic corticosteroids are required if there is severe swelling of the throat, which hazards the airway.
Nearly 20% of patients have concurrent beta-hemolytic streptococcal throat infection, for which penicillin may be given.
Tinidazaole may improve the sore throat.
Good post and this fill someone in on helped me alot in my college assignement. Gratefulness you for your information.
I never thought that I would learn so much from this post. This contains very substantial information that must be known to all of us so that we can prevent the spread of this type of disease. Great post, thank you for this!
Thank you for sharing this informative article. This is why regular habits of oral hygiene should be practiced to avoid infection and worsening of existing sores.
Great information! I’ve been looking for something like this for a while now. Thanks!
Very nice article. Very informative. Thank you for sharing.
Keep posting stuff like this i really like it