A thyroglossal cyst is a fibrous cyst that forms from a persistent thyroglossal duct.
Presentation
It usually presents as a midline neck lump (in the region of the hyoid bone) that is usually painless, smooth and cystic, if infected pain can occur. There may be difficulty breathing, dysphagia (difficulty swallowing), and/or dyspepsia (discomfort in the upper abdomen), especially if the lump becomes large.

Thyroglossal duct cyst present as swelling in the midline of the neck
The most common locations for a thyroglossal cyst are midline or slightly off midline, between the isthmus of the thyroid and the hyoid bone or just above the hyoid bone. A thyroglossal cyst can develop anywhere along a thyroglossal duct, though cysts within the tongue or in the floor of the mouth are rare.
A thyroglossal cyst will move upwards with protrusion of the tongue.
Thyroglossal cysts are associated with an increased incidence of ectopic thyroid tissue. Occasionally, a lingual thyroid can be seen as a flattened strawberry-like lump at the base of the tongue.
Embryology
The thyroglossal tract arises from the foramen cecum at the junction of the anterior two-thirds and posterior one-third of the tongue. Any part of the tract can persist causing a sinus, fistula or cyst. Most fistulae are acquired following rupture or incision of the infected thyroglossal cyst.
Symptoms
Thyroglossal duct cysts most often present with a palpable (able to be felt) asymptomatic midline neck mass below the level of the hyoid bone. The mass on the neck moves during swallowing or on protrusion of the tongue because of its attachment to the tongue via the tract of thyroid descent. Some patients will have neck or throat pain, or dysphagia.
The persistent duct or sinus can promote oral secretions, which may cause cysts to become infected. Up to half of thyroglossal cysts are not diagnosed until adult life. The tract can lie dormant for years or even decades until some kind of stimulus leads to cystic dilation. Infection can sometimes cause the transient appearance of a mass or enlargement of the cyst, at times with periodic recurrences. Spontaneous drainage may also occur.
Clinical features

Thyroglossal duct cyst present as a swelling in the midline of the neck
Clinical features can be found in the subhyoid portion of the tract and 75% present as midline swellings. The remainder can be found as far lateral as lateral tip of the hyoid bone.
Typically, the cyst will move upwards on protrusion of the tongue, given its attachment to the embryonic duct.
How is a thyroglossal duct cyst diagnosed?
Generally, diagnosis is made by physical examination. The mass typically moves upward when the tongue is extended and with swallowing since the thyroglossal duct often connects at the base of the tongue. It is important to determine if the thyroglossal duct cyst contains thyroid tissues. In addition to a complete medical history and physical examination, diagnostic procedures for a thyroglossal duct cyst may include the following:
- blood tests (to assess thyroid function)
- ultrasound examination – to evaluate the muscle around the mass; a diagnostic imaging technique which uses high-frequency sound waves and a computer to create images of blood vessels, tissues, and organs. Ultrasounds are used to view internal organs as they function, and to assess blood flow through various vessels.
- thyroid scans – a procedure that uses radioactive iodine or technetium (a radioactive metallic element) to reveal any physical abnormalities of the thyroid.
Treatment

Thyroglossal duct cyst (pointed by arrow) as seen on CT scan
Specific treatment of a thyroglossal duct cyst will be determined by your child’s physician based on:
- your child’s age, overall health, and medical history
- extent of the condition
- your child’s tolerance for specific medications, procedures, or therapies
- expectations for the course of the condition
- your opinion or preference
Treatment may include:
- antibiotic medication (to treat the infection)
- surgical removal of the cyst and the thyroglossal duct, called the Sistrunk procedure
For a thyroglossal cyst is surgical resection, often requiring concomitant removal of the midsection of the hyoid bone (Sistrunk procedure), to prevent recurrence. Although generally benign the cyst will be removed if the patient exhibits difficulty in breathing or swallowing, or if the cyst is infected. Even if these symptoms are not present the cyst may be removed to eliminate the chance of infection or development of a carcinoma, or for cosmetic reasons if there is unsightly protrusion from the neck.
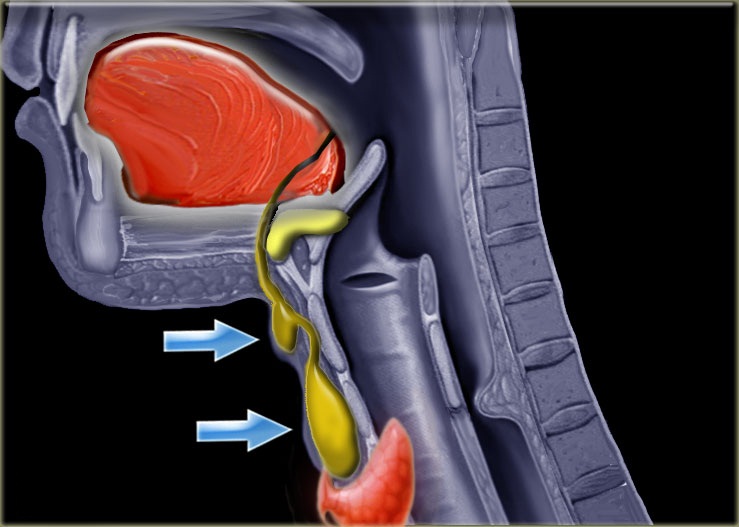
The thyroglossal duct runs from the posterior part of the mouth to the neck
The Sistrunk procedure involves excision not only of the cyst but also of the path’s tract and branches. A removal of the central portion of the hyoid bone is indicated to ensure complete removal of the tract. It is unlikely that there will be a recurrence after such an operation. The original Sistrunk paper is available on-line with a modern commentary. At times antibiotics can be indicated if there is sign of infection.
Thyroid scans and thyroid function studies are ordered preoperatively; this is important to demonstrate that normally functioning thyroid tissue is in its usual area.