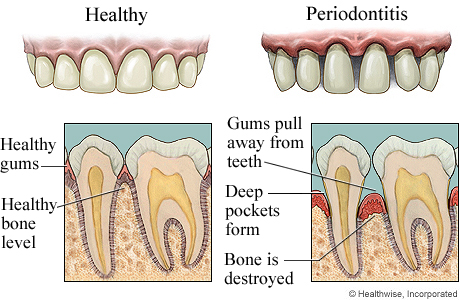
 Periodontal disease involves the peridontium consisting of the gums, alveolar or jaw bone, the periodontal ligament and the cementum of tooth. Therefore it is of no surprise if the disease leads to bone defects in our jaw bone or cause furcation involvement.
Periodontal disease involves the peridontium consisting of the gums, alveolar or jaw bone, the periodontal ligament and the cementum of tooth. Therefore it is of no surprise if the disease leads to bone defects in our jaw bone or cause furcation involvement.
What are bone defects?
Bone or osseous defects are concavities or deformities in the alveolar bone involving one or more teeth. All procedures designed to modify and re-shape defects and deformities in the bone surrounding the teeth are called osseous surgery. The most common pattern of bone loss is reduction in height of bone.
What is furcation involvement?
Furcation involvement is a condition in which bifurcation and trifurcations of multi-rooted teeth (the areas where the tooth root splits) are invaded by periodontal disease process.
What is the purpose of treatment of bone defects and furcation involvement?
The objectives of treatment of these defects are:
- To eliminate the periodontal lesion
- To achieve a tissue shape that will allow efficient plaque control
- To obtain some bone formation, new attachment and improve tooth support
What causes bone defects and furcation involvement?
© pinnaclepediatricdentistry.com
Bone defects and furcation involvement is a consequence of untreated periodontitis. Dental plaque is the major cause of periodontitis. Persistent infection of the gum margins leads to progressive inflammation and destruction of the supporting tissues by bacterial toxins and enzymes. Extension and the hardening of plaque lead to formation of tartar beneath the gums. Having tartar within the gum pockets can lead to periodontitis. It forms a reservoir of bacteria which help to keep inflammation and acts as a barrier to healing. The following risk factors can increase the chances of having periodontitis:
Risk factors for periodontal disease
Local factors
- Alignment and the bite relationship of teeth
- Faulty fillings of teeth
- Mouth breathing
- Dentures or braces
- Smoking
- Diabetes mellitus
- Pregnancy
- Nutrition deficiency
- Blood diseases
- Drugs
- HIV infection
Classification of Bone defects
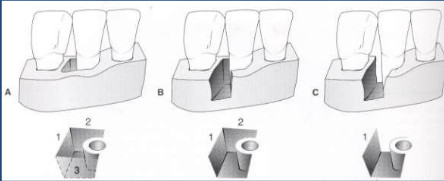
- One wall defect – usually only one interdental wall remains and is called hemi septum if remaining wall is proximal. Poor prognosis for periodontal regeneration since it is difficult to stabilize the graft material to be used in its proper place.
- Two wall defect – most prevalent bone defect found interdentally with facial and lingual walls remaining, involves both the interproximal walls which are mainly called crater defects or interdental crater defects.
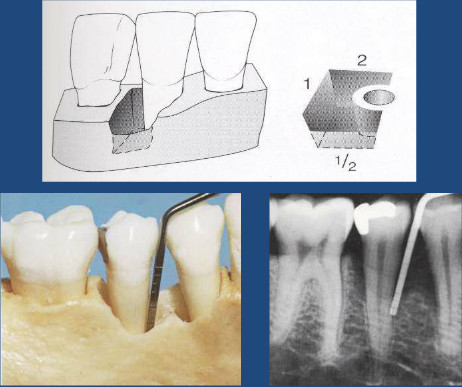
- Three wall defect – occurs most frequently in the interdental region, usually the remaining bony walls are facial, lingual and proximal can be circumferential defects. The ideal osseous defect for a regenerative procedure as this defect shape will favor the stabilization of a graft material to be used.
 Combined defect – combination of one, two or three wall defect
Combined defect – combination of one, two or three wall defect- Fenestration – isolated areas in which the root is denuded of bone and the root surface is covered only by periosteum and overlying gums. Marginal bone is intact
- Dehiscence – areas where the defect extends through the marginal bone
Classification of furcation involvements
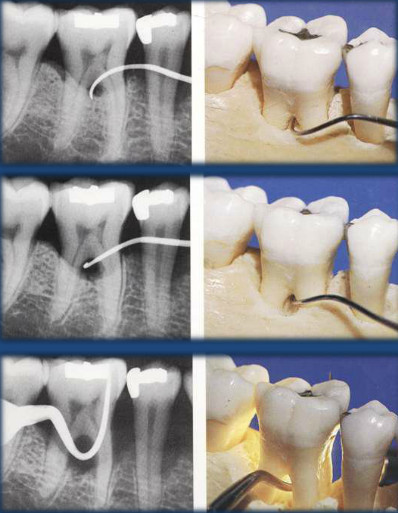
The classification was introduced by Glickman in 1953, and a Nabers probe is used for diagnosis of tooth furcation involvement.
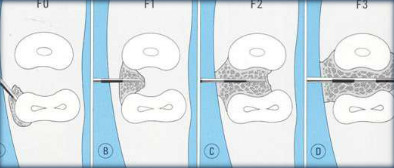 Grade I involvement – also known as incipient or early lesion, there is slight bone loss in the furcation area and usually no x-ray or radiographic findings are present.
Grade I involvement – also known as incipient or early lesion, there is slight bone loss in the furcation area and usually no x-ray or radiographic findings are present.
- Grade II involvement – bone destruction is present and there is partial penetration of probe into furcation area. The lesion is also known as cul-de-sac (A passage with access only at one end) and x-ray or radiograph may or may not show changes.
- Grade III involvement – interradicular bone (the bone between the roots of tooth) is completely lost but the defect is covered by gums therefore the furcation is not visible clinically. There is a radiolucent area seen between the roots in lower molars in the x-ray or radiograph.
- Grade IV involvement – interradicular bone is completely destroyed, gums are receded and the furcation of tooth is clinically visible.
What is the treatment of furcation involvement?
The aim of furcation treatment:
- To expose the furcation (to provide assess for cleaning)
- To induce regeneration of new bone
Grade I furcation involvement (early lesion)

- Scaling and curettage followed by maintenance
- Gingivectomy or apical positioning of the flap
- Bone reshaping
- Reshaping the tooth (odontoplasty)
Grade II furcation involvement
One aspect is intact in Grade II furcation therefore treatment is performed from the involved side.
- Granulation tissue removed, scaling and root planning
- Osseous repair with bone grafts and guided tissue regeneration (GTR)
- Gingivectomy (removal of gum tissues) or apical positioning of flap
- After healing maintained with single tufted brush
Grade III and IV furcation involvement
 Grade III and IV are through and through defects in which the probe passes freely through the defect.
Grade III and IV are through and through defects in which the probe passes freely through the defect.
Techniques
- Simple exposure by gingivectomy or apical reposition flap
- Tunnel preparation for lower molars to provide space for spiral brush to pass freely
- Root resection or root amputation (removal of the root without removal of any portion of the crown)
- Hemisection (when one root and the corresponding crown portion are cut and removed)
- Bicuspidization (lower molar is cut into two separate mesial and distal portion, without removal of any part of the root or crown)
- Extraction ensures removal of periodontal disease but carries its own problems.
All procedures are accompanied by removal of granulation tissue, scaling and root planing, bone contouring and maintenance after healing.
To be continued in Part 2