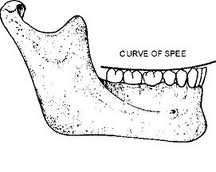
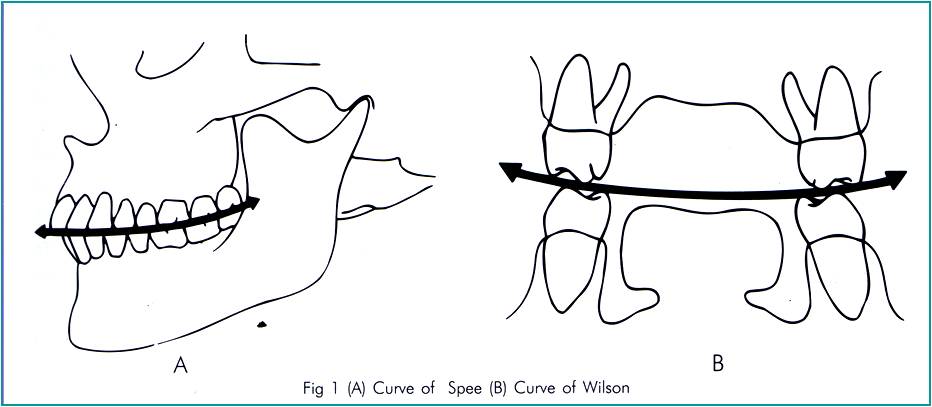
In Anatomy, the Curve of Spee (called also von Spee’s curve or Spee’s curvature) is defined as the curvature of the mandibular occlusal plane beginning at the tip of the lower cuspid and following the buccal cusps of the posterior teeth, continuing to the terminal molar. According to another definition Curve of Spee is an anatomic curvature of the occlusal alignment of teeth, beginning at the tip of the lower canine, following the buccal cusps of the natural premolars and molars, and continuing to the anterior border of the ramus. Ferdinand Graf von Spee, German embryologist, (1855–1937) was first to describe anatomic relations of human teeth in the sagittal plane.
 The pull of the main muscle of mastication, the masseter, is at a perpendicular angle with the curve of Spee to adapt for favorable loading of force on the teeth.
The pull of the main muscle of mastication, the masseter, is at a perpendicular angle with the curve of Spee to adapt for favorable loading of force on the teeth.
The Curve of Spee is, essentially, a series of slipped contact points. It is of importance to orthodontists as it may contribute to an increased overbite. Larry Andrews, in his important paper: Six Keys to Normal Occlusion (1972), stated that a flat or mild curve of Spee was essential to an ideal occlusion.
The curve of Spee should not be confused with the curve of Wilson, which is the upward (i.e. “U†shaped) curvature of the maxillary and mandibular occlusal planes in the coronal plane.
Orthodontists do not evaluate and consider the Curve of Spee in all cases, treatment planning should be a combination of cephalometric analysis and dental discrepancy but consideration of the curve of Spee is an important factor in diagnosis. Although leveling the curve of Spee is an everyday occurrence in orthodontic practice, little research has been dedicated to the examination of the relationship between the depth of the curve of Spee and different malocclusions. In a study that was conducted, therefore, the relationships between the depth of the curve of Spee in class I, class II div 1 and 2, class II subdivision and class III malocclusion have been evaluated.

Normal depth of Curve of Spee: 2-3 mm
In this study the gender of the subjects had no significant effect on the variables assessed which confirms previous reports of the absence of sexual dimorphism in the curve of Spee in class I, II and III malocclusions.
The study results showed that depth of curve of Spee was deepest in class II div 2 malocclusion and was flat in class III malocclusion suggesting that the curve of Spee in mandibular arch is influenced by the anterioposterior position of the mandible. This coincides with the previous reports that the radius of curve of Spee is shorter in those with class II malocclusion than class III malocclusion.
The amounts of overbite and over jet significantly influence the variation of the curve of Spee in the mandibular arch. The depth of the curve of Spee in the mandibular arch increases with an increase in over jet and overbite. The results obtained from the study confirmed the above finding as depth of curve of Spee increases in class II div 1 and 2 malocclusions in which there are increase overjet and overbite. Trauten et al and Orthlieb reported that there was a negative curve of Spee in open-bite cases, whereas a deep curve of Spee in deep-bite cases was found. On the other hand, Farella et al found that the curve of Spee is more marked in short-face subjects and less marked in long-face subjects. Similarly, we found that the curve of Spee is deepest in class II div 2 malocclusions that have deep overbite and short face heights (Low angle) than in the normal and flat Spee groups and it was flat in class III malocclusion that have both high and low angle variants.
 Shannon and Nanda found that Class II malocclusion had significantly deeper pretreatment curve of Spee measurements than Class I malocclusions and same is the case in our study. The curve of Spee contributes to set up the anterior overbite and is favorable to the approach of the maxillary and mandibular occlusal planes, in mandibular elevation. According to this concept, the curve of Spee depth in individuals with Class II malocclusion should be deeper than in individuals with clinically normal occlusion. Andrews also suggested that one of the six keys to normal occlusion is the existence of a leveled occlusal plane or a mild curve of Spee, which was observed in the present study, with a mean value of 1.01 mm to the curve of occlusal plane. An excessive overbite can be an indication of incorrect curve of Spee; in the same way, an exaggerated curve of Spee can be accompanied by an increased overbite.
Shannon and Nanda found that Class II malocclusion had significantly deeper pretreatment curve of Spee measurements than Class I malocclusions and same is the case in our study. The curve of Spee contributes to set up the anterior overbite and is favorable to the approach of the maxillary and mandibular occlusal planes, in mandibular elevation. According to this concept, the curve of Spee depth in individuals with Class II malocclusion should be deeper than in individuals with clinically normal occlusion. Andrews also suggested that one of the six keys to normal occlusion is the existence of a leveled occlusal plane or a mild curve of Spee, which was observed in the present study, with a mean value of 1.01 mm to the curve of occlusal plane. An excessive overbite can be an indication of incorrect curve of Spee; in the same way, an exaggerated curve of Spee can be accompanied by an increased overbite.
The clinical evaluation should be associated and considered in orthodontic treatment planning. One of the orthodontic treatment purposes is leveling the curve of Spee and for this leveling, the value of the curve of Spee depth should be considered and quantified in space management procedures to prevent incisor flaring and consequently assuring aesthetics, stability of the treatment results and function. Analysis of the curve of Spee might assist dentists in determining the sagittal organization of the teeth. The curve of Spee can be used as a reference for prosthetic restoration and orthodontic treatment. Management of the curve of Spee is critical for achieving stability of complete dentures and could play a role in the success of implant-supported restoration.