WORKING LENGTH DETERMINATION
In detail endodontic procedure primarily consists of
-        Access preparation –LA in vital
-Â Â Â Â Â Â Â Â Pulpectomy
-Â Â Â Â Â Â Â Â Working length X-ray
-Â Â Â Â Â Â Â Â Biomechanical preparation (cleaning and shaping)
Chemo-mechanical preparation disinfection
Obturation
Steps in endodontic Rx
Ø     Exploring
Ø     Extirpating
Ø     Cleaning and shaping
Ø     Obturation
Local anaesthesia: given in vital teeth
 – Â Â Â Â Infiltration anaesthesia
– Â Â Â Â Infiltration anaesthesia
-Â Â Â Â Â Â Â Â Block anaesthesia
-Â Â Â Â Â Â Â Â Intrapulpal anaesthesia
-Â Â Â Â Â Â Â Â Intra ligamentary anaestesia

After access Preparation ( Tooth with 2 canals)
 Exploring the Root Canal:

Once access preparation is over then explore the canal with smooth broach to confirm the patency of root canals
Extirpation of pulp or pulpectomy
Is to remove pulp from pulp chamber and root canals. Pulp chamber and root canal may contain a partially vital or necrotic pulp
When pulpectomy is done, pulp in literally torn. This procedure leaves a lacerated wound,and the reaction at the apex comprises of haemorrhage, inflammation and repair.
In anterior teeth, that are vital, it’s necessary to remove the pulp in toto , otherwise RBCS will rupture and iron content gets diffused into dentinal tubules and causes discoloration of tooth.
Working Length Determination
Definition:
Working length in defined as length at which instrumentation should be limited and subsequent obturation completed.
Significance of calculating Working Length:
It determines how far into the canal the
instruments are placed and worked.
It will limit the depth to which the canal filling
may be placed.
It affects the degree of pain and discomfort
the patient feels following the appointment.
It also determines the success of the treatment.
ANATOMICAL CONSIDERATIONS AND TERMINOLOGY
Simon has stressed the use of terms related to working length determination.
WORKING LENGTH: –
DEFINITION: – “The distance from a coronal reference point to the point at which canal preparation and obturation should terminateâ€. The ideal apical reference point in the canal is “apical stopâ€.
ANATOMIC APEX: – Is the tip (or) the end of the root determined morphologically.
RADIOGRAPHIC APEX: -Is the tip (or) the end of root determined radiographically.
APICAL FORAMEN: – Is the region where the canal leaves the root surface next to the periodontal ligament.
It is frequently eccentrically located away from the anatomic (or) radiographic apex. The anatomy of apical foramen changes with age. (a) The concept of the apex (b) The apex of a younger person (c) changing apex due to hard tissue deposition.
ACCESSORY FORAMEN: – Is an orifice on the surface of the root communicating with a lateral (or) accessory canal. They may exist as a single foramen (or) as multiple foramina.
APICAL CONSTRICTION: – (Minor diameter) is the apical portion of the root canal having the narrowest diameter. The minor diameter widens apically to the foramen (major diameter) and assumes a funnel shape
The funnel tapers to a distance short of the site of exiting and widens again. Because the adjacent walls of cementum are slightly convex (or) hyperbolic it resembles that of a morning glory flower.
THE CEMENTODENTINAL JUNCTION (CDJ):– Is the region where the dentin and cementum are united, the point at which the cemental surface terminates at (or) near the apex of a tooth. The CDJ is a histological landmark and cannot be located radio graphically (or) clinically.
Location of CDJ is 0.5 to 3.0mm short of the anatomic apex
ENDOMETRY: The term endometry refers to the accurate determination of the working length, which decides the apical termination part for all inter canal procedures from a reference point.
Methods of determining working lengths
1) Â Â Â Radiographs
Digital monitoring systems (RVG)
2)Â Â Â Â Â Electronic method.
3)Â Â Â Â Â Audiometric method
4)Â Â Â Â Â Tactile Sense
5)Â Â Â Â Â Patient response
6)Â Â Â Â Â Paper point measurement.
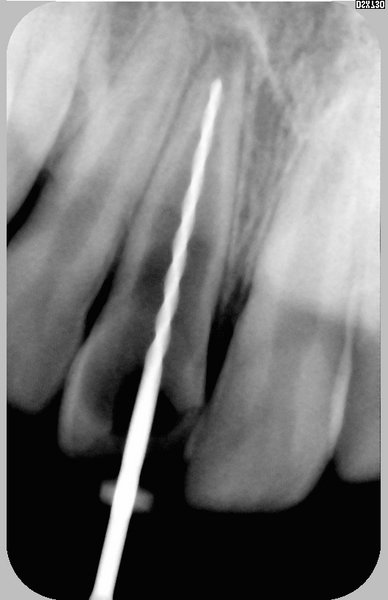
Radiographs
Play a very important role in BMP since it permits the operator to form a visual conception of internal tooth structure.
Radiograph is an exact “road map†of anticipated journey between access opening into the pulp chamber and the apical foramen.
Radiographs provides an information about length, curvature, number of canals and also presence of multiple canals in single roots and also about lateral and accessory canals
Presence of calcifications,perforations obstructions and peri apical lesions may be known.
It also provides the presence of atypical anatomy like apical bifurcations and complexities.
Reference points
In anterior’s – incisal edges
In posterior’s -cusp tips In anterior teeth the reference point is usually the incisal edge, but broken down teeth may be measured from adjustment teeth (or) from some projecting portion of the remaining tooth structure
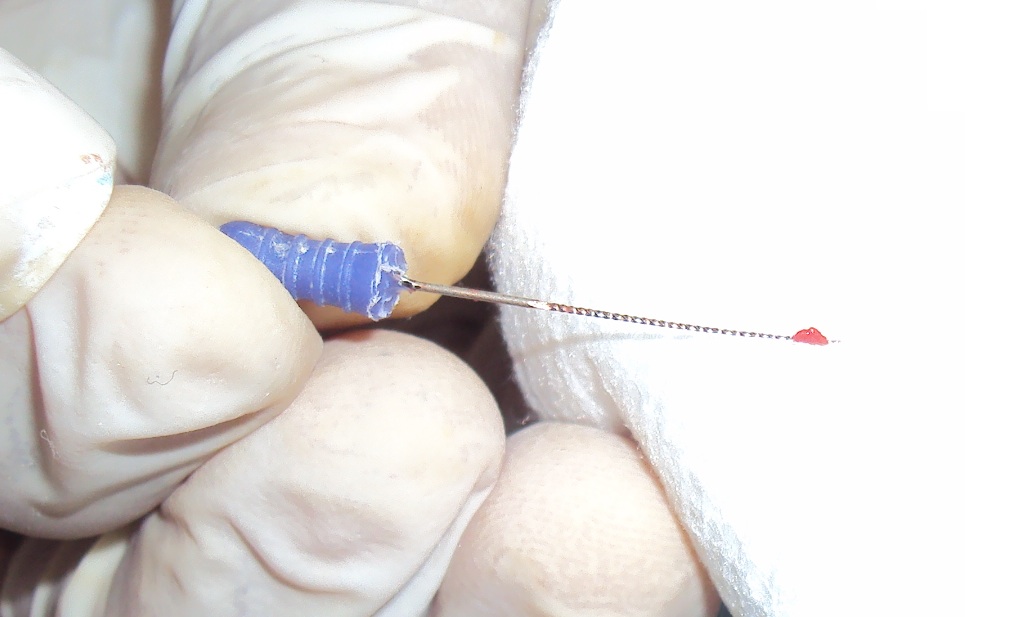
Instruments used
– Usually 20 no. K-files
-Â In multi-rooted teeth, can use different instruments in different canals
Ex- K-file and Reamers.
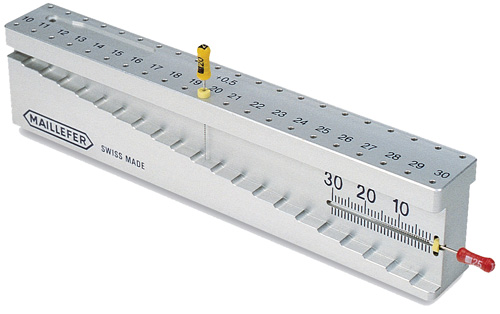
STOP ATTACHMENTS
The setting of an instrument to exact W.L is important as it confirms instrument to a R.C and it prevents over extension.
It can be done by using stoppers:
Rubber or silicone or
plastic stops
Metal stops