Pulpotomy
Definition
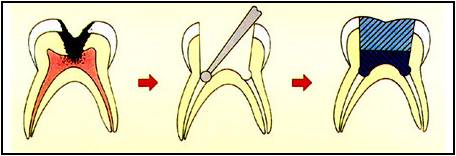
Pulpotomy is defined as the amputation of damaged and inflammed vital pulp from the coronal chamber followed by placement of a medicament over the radicular pulp stumps to stimulate repair, fixation or mummification of the remaining vital radicular pulp.
– Braham & Morris 1985
Pulpotomy is defined as the surgical removal of infected coronal pulp and its objectives are preservation of the radicular pulp vitality and relief of pain.
Rationale of Pulpotomy
When the coronal pulp is exposed due to caries, trauma or operative procedures. It produces inflammatory changes in the pulp.
Through the surgical excision of the coronal pulp the infected and the inflamed area is removed leaving vital, unaffected pulpal tissue in the root canal well preserved.
This efforts in temporary and rapid relief of pulpalgia and the unaffected tissue undergoes repair.
History
The Europeans were the first to introduce pulpotomy procedure.
1885 – Leptowski: introduced formalin as fixative and mummifying agent.
1886 – Gold foil was used to cover the exposed vital pulp.
1898 – Gysi: Introduced paraformaldehyde as a pulpotomy medicament.
1904 – Buckley: Introduced formocresol for pulpotomy.
1930 – Hermann: Introduced calcium hydroxide as calxyl for pulpotomy.
1975 – S’Gravemade: used gluteraldehyde which replaced formocresol.
1983 – Reumping et al: demonstrated the use of electrosurgery for pulpotomy.
1985 – Shoji: used carbon dioxide laser in pulpotomy.
1991 – Nakashima used bone morphogenic protein.
1993 – Torabinejad: MTA was used
Classification
Pulpotomy can be classified according to treatment objectives (Don M. Ranly 1994).
1.Devitalization pulpotomy (Mummification, cauterization)
Formocresol pulpotomy
Electrosurgical pulpotomy
Laser pulpotomy
2. Preservation (minimum devitalization, non inductive)
Gluteraldehyde
Ferric sulfate
3. Regeneration (Inductive & Reperative)
Calcium hydroxide
Bone morphogenic protein
Depending upon the size of exposure
1. Partial pulpotomy (shallow, low level or Cvek’s pulpotomy)
2. Cervical pulpotomy (deep, high level total or conventional pulpotomy)
Classified depending upon the number of visits
1. Single visit pulpotomy
2. Multiple visit pulpotomy
Indications
Mechanically exposed vital primary teeth.
Caries exposure in vital asymptomatic primary tooth
In the treatment of pulpally involved primary teeth with clinical manifestations of inflammation confined to coronal pulp.
In the treatment of pulpally involved permanent teeth with open apices and vital pulp.
In the treatment of fracture permanent teeth with pulp exposure >1sqmm.
Contraindications
Spontaneous pain
Abnormal sensitivity to heat or cold / chronic pulpalgia
Tenderness to percussion
Swelling / sinus
Pus or serous exudates at the exposure site
Pathological mobility
Uncontrolled hemorrhage from the amputated pulp stumps
Pathological external root resorption
Periapical or inter radicular radiolucency
Internal root resorption
Pulp calcification / constriction of pulp chamber
Materials Used By Dentists
Formocresol
Gluteraldehyde
Devitalizing paraformaldehyde paste
Gysi paste
Easlicks paraformaldehyde paste
Paraform devitalizing paste
Camphorated paramonochlorophenol
Cresol
Metacresyl acetate
Oxypara
N2 Compound
Zinc oxide eugenol
Ferric sulphate
Calcium hydroxide
Enriched collagen solution
Collagen calcium phosphate gel
Dimethyl subirridemate
Tetrandrine
Freeze dried bone
Tricalcium phosphate
Chondritin sulfate
Sodium hydluronate
Dinatured albumin
Pure calcium hydroxide apatite
Antibiotic paste
MTA
Dentin bonding agent
Bone morphogenic protein
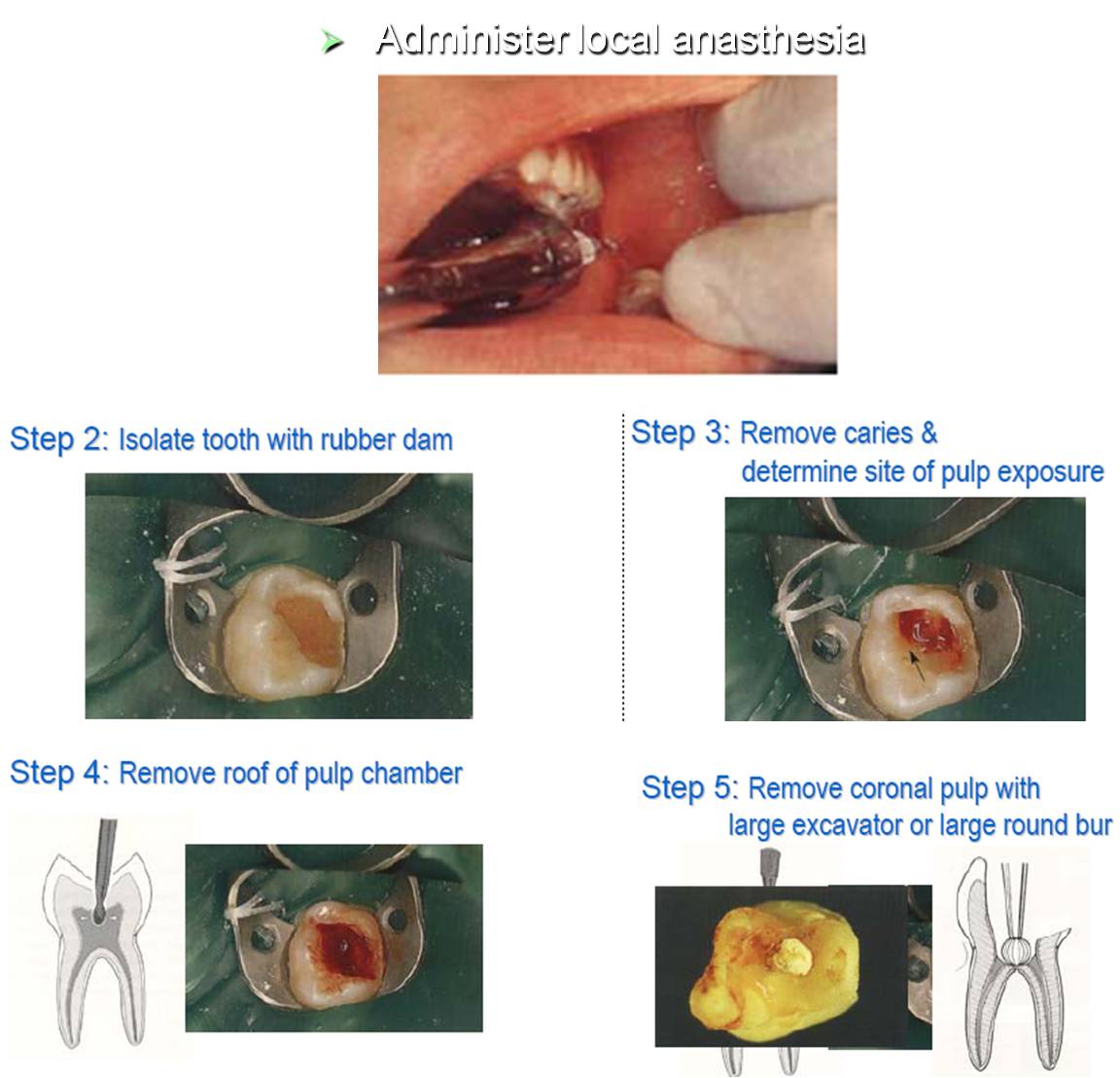
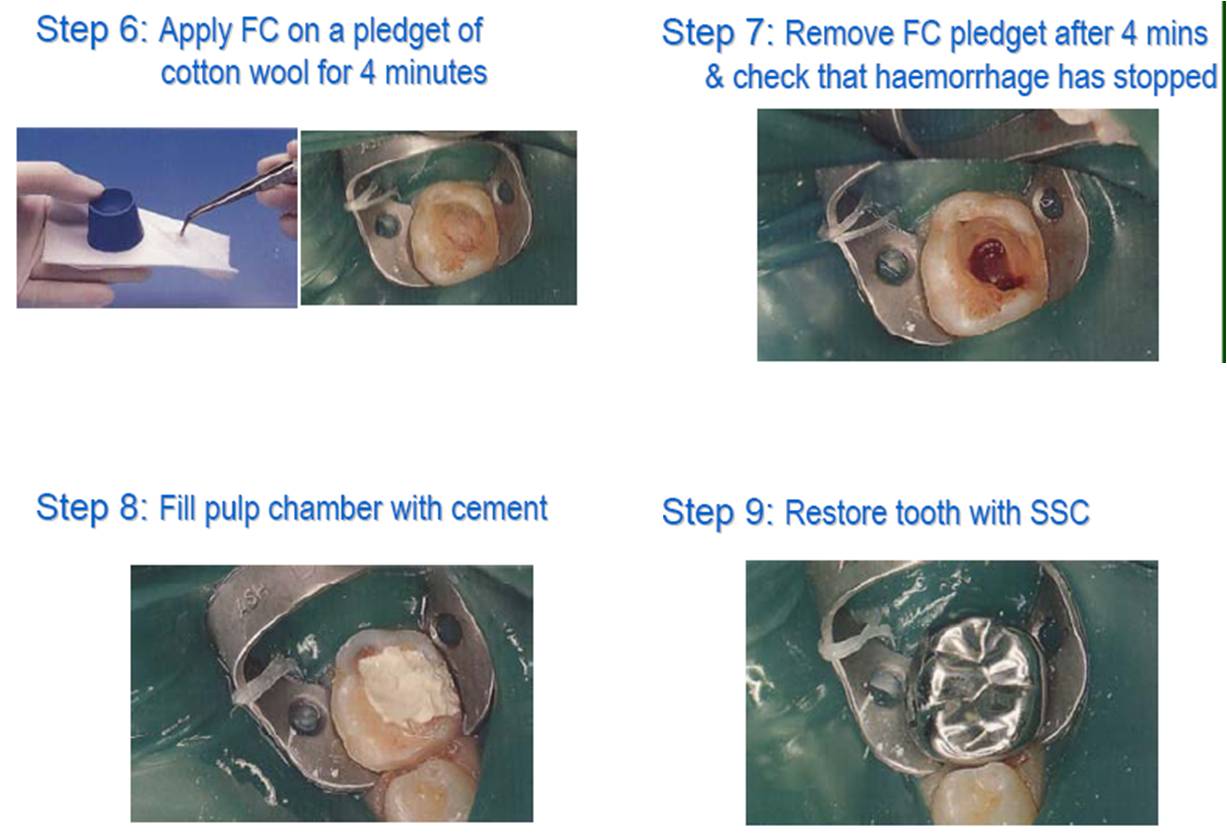
What Does The Dentist Do To Your Teeth?
Types of Pulpotomies
Non-vital pulpotomy (mortal pulpotomy)
Electrosurgical pulpotomy
Laser pulpotomy
Preservation pulpotomy
Gluteraldehyde.
Ferric sulphate
Partial / Cvek’s pulpotomy
Cervical –Webbers pulpotomy
Regenerative pulpotomy
Apexogenesis & Apexification
Open apex
At the time of tooth eruption root development is only 62-80% i.e., 2/3rd of the root is formed.
If due to trauma or caries exposure the pulp undergoes necrosis, dentin formation ceases and root growth is arrested.
The resultant immature root will have an open apex which is also called as blunder buss canal.
Problems faced with open apex
due to large apical diameter and smaller coronal canal diameter debridement is difficult.
Lack of apical stop makes obturation difficult.
The thin root canal walls become prone to fracture.
Earlier open apices have been treated by periapical surgery with a retrograde filling but surgery has its drawbacks.
Relative to the already shortened root, further root reduction (apicectomy) could result in an inadequate crown root ratio.
The apical walls are thin and could shatter when touched with a rotating bur.
The thin walls would make condensation of a retrograde filling difficult.
The periapical tissue may not adapt to the wide and irregular surface of the amalgam.
Surgery would remove the root sheath and prevent for further root development.
Surgery would be both physically and psychologically traumatic to the patient.
Thus It is best to treat immature teeth with a non surgical approach.
Based on the vitality of the pulp if the immature tooth has vital pulp exhibiting reversible pulpitis physiological root end development or apexogenesis is attempted.
If irreversible pulpitis is present there is when pulp is necrotic then root end closure is done by apexification.