© soms.com.au
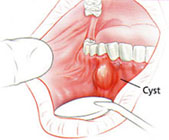
A cyst is defined as a pathological cavity having fluid or semi-fluid contents, which has not been created by the accumulation of pus. Cysts of the jaws are more common than in any other bone, and the majority are lined wholly or in part by epithelium.
Basic treatment goals
- Eradication of pathology – Removal of entire lesion and prevention of recurrence.
- Functional rehabilitation – The defect after surgery can vary therefore the method of reconstruction should be evaluated and decide before surgery.
How to treat a jaw cyst
- Enucleation
- Marsupialization
- Combination of both
- Enucleation with curettage
Enucleation
Enucleation means shelling out the entire cystic lesion without rupture. This procedure is usually indicated for a small cyst, which can be done when the vital structures are not involved.
Technique
- Local anesthesia is administered.
- The gum flap of the concerned region is lifted.
- Tooth extractionof the involved tooth is done.
- If needed, a window through the jaw bone is created for access.
- A thin blade curette is used to cleave the cystic lining from the bony cavity.
- The socket is inspected and any remnants are removed.
- A water tight closure is done.
- Eventually this cavity, filled with blood, gets organized into bone.
- For large cyst cavities, external pressure dressing is given and is removed after 24 to 48 hours to reduce swelling and the size of the blood clot.
- Formation of bone takes place in 6 to 12 months.
Marsupialization
Marsupialization refers to creating a surgical window in the wall of the cyst, excavating the contents of the cyst and maintaining continuity between the cyst wall and the oral cavity. Only a portion of the cyst is removed with the remaining left in situ. This process decreases the pressure inside the cyst, and promotes shrinkage of the cyst as well as bone fill.
Indications
- Amount of tissue injury – depends on the proximity of cyst to vital structures, possibility of injury to nerve.
- Surgical access – if difficult.
- Assistance in eruption of teeth – if an unerupted teeth is involved in the cyst and is needed in the mouth.
- Extent of surgery – in an unhealthy or feeble individual.
- Size of cyst – very large cyst or risk of pathological fracture of bone
Advantages
- Simple procedure to perform
- Spare vital structures from damage
Disadvantages
- Pathological or diseased tissue is left inside
- Inconvenience for the patient – cavity should be kept clean from food debris, saline irrigation has to be done several times a day and this may continue for several months until there is evidence of bone formation in the cystic cavity.
Technique
- After local anesthesia is administered, the cystic cavity is aspirated with a syringe.
- If the aspiration confirms of cystic contents, then an incision is made to create a large window into the cystic cavity.
- The cystic cavity is irrigated with saline solution.
- The residual cyst is examined – If areas of ulceration or thickening are present, tumor changes in the wall of the cyst is suspected and in this case, a biopsy of the suspicious area is done. If the cystic lining is thick, the perimeter of the cystic wall is stitched with the soft tissues in the mouth.
- The cavity is packed with lincture of benzoin or whitehead varnish.
- The pack is left in place for 10 to 14 days and careful instructions regarding cleansing of the cavity will be given.
- The cavity will be repacked continuously until it contracts.
- Once tissue growth takes place, the pack is replaced with a semi rigid acrylic plate.
- At this stage the individual can wash out the cavity after every meal until the cavity closes.
Combination of both
Combined approach reduces morbidity and hastens complete healing of the defect. In this technique marsupialization is done first and the enucleation is done at a later date. The advantage is that as marsupialization is done first, it spares the vital structures. The size of the cystic cavity also becomes small and after healing the cystic lining becomes thick, making enucleation easier at this stage.
Enucleation with curettage
After enucleation is done, a curette or bur is used to remove 1 to 2 millimeter of bone around the entire periphery of cystic cavity.
Indications
- For cysts reported to have high recurrence rate, for example odontogenic keratocyst
- Any cyst that recurs after its initial removal
Advantages
If enucleation leaves any remnants, curettage may remove them thereby decreasing the likelihood of recurrence.
Disadvantage
Curettage is more destructive to adjacent bone, blood vessels and nerves therefore extreme care has to be taken to prevent this.
Wow, thank you. This quick and easy explanation is just what I need. It would’ve been better though if you attached bibliography. But thank you, really.