Numerous risk indicators, that is, characteristics or measurements that assist in the prediction of caries, whether or not they are involved in caries causation, have been suggested for children. Unfortunately, more of the supportive data come from cross-sectional correlations with accumulated caries experience than from prospective, protocol-based incidence studies. The prospective studies employed different combinations of potential predictors in a variety of populations, varied considerably in sample size and quality, and have not produced a broadly applicable index or set of criteria for risk assessment. More and higher-quality comprehensive, longitudinal, multifactor studies of implicated risk indicators are needed to obtain firm support for their associations with caries incidence, to clarify the strengths of these associations in differing populations, and to reveal the extent to which the risk indicators provide independent as opposed to redundant information. In addition, although the nature of the disease process suggests that many of the proposed indicators may well be appropriate throughout life, validation studies in adult populations are largely absent or incomplete.

Nevertheless, in practice there are several readily determinable indicators that together provide helpful guidance when dealing with otherwise healthy persons and some well-validated medical or disability conditions that place individuals at heightened caries risk.
Thus far, the most consistent predictor of caries risk in children is past caries experience. In addition, there is evidence of matrilineal transmission of mutans streptococci in early childhood. Hence, the presence of caries in the mother and siblings increases risks for the child.
Regular brushing of tooth surfaces using a fluoride-containing dentifrice, reduces caries risk. Conversely, inadequate exposure to fluoride confers increased risk. Conditions that compromise the long-term maintenance of good oral hygiene are also positively associated with caries risk. These include certain illnesses, physical and mental disabilities, and the presence of existing restorations or oral appliances.
Fermentable carbohydrate consumption fuels acid formation and demineralization and is associated with caries, particularly in the absence of fluoride. The amount, consistency, and frequency of consumption determine the degree of exposure. Long-term regular doses of medications containing glucose, fructose, or sucrose may also contribute to caries risk.
Medical conditions such as Sjogren’s syndrome, pharmacological agents with xerostomic side effects, and therapeutic radiation to the head and neck, lower salivary flow rate to pathological levels and dramatically elevate a patient’s risk of caries. This suggests that normal salivary flow rate is protective against caries. Some studies indicate that low buffering capacity, low salivary IgA, and low salivary calcium and phosphate are weakly linked to increased caries as well.
Mutans streptococci
Mutans streptococci is an established etiologic agent for caries, and its presence clearly indicates the potential for cariogenic activity. However, its presence alone is no more than weakly predictive of clinical caries activity.
While some of the risk indicators known for children may well be applicable across all ages, some may differ across ages in the way they act or in their degrees of importance, while other risk indicators must be considered distinctive for adult and elderly populations. Thus, the inability to maintain good oral hygiene and xerostomia are risk factors of special significance among the elderly, and gingival recession uniquely increases the risk of root caries in elderly populations by exposing previously protected root surfaces to cariogenesis.
Low indices of socioeconomic status (SES) have been associated with elevations in caries, although the extent to which this indicator may simply reflect previous correlates is unknown. Low SES is also associated with reduced access to care, reduced oral health aspirations, low self-efficacy, and health behaviors that may enhance caries risk.
Caries is an etiologically complex disease process. It is likely that numerous microbial, genetic, immunological, behavioral, and environmental contributors to risk are at play in determining the occurrence and severity of clinical disease. Assessment tools based on a single risk indicator are therefore unlikely to accurately discriminate between those at high and low risk. Multiple indicators, combined on an appropriate scale and accounting for possible interactions, will certainly be required.
3. How should clinical decisions regarding prevention and/or treatment be affected by detection methods and risk assessment?
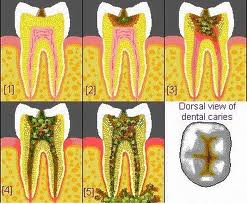
Progression of dental caries
At this time the panel senses a paradigm shift in the management of dental caries toward improved diagnosis of early noncavitated lesions and treatment for prevention and arrest of such lesions. Restorations repair the tooth structure, do not stop caries, and have a finite life span. They are themselves susceptible to disease. With the defining of caries as a multifactorial, multistage process extending from infection to demineralization and cavitation, clear diagnostic and staging criteria as well as a clear understanding of risk and prognosis are needed to determine dental treatment options. Evidence suggests that there are nonsurgical options for prevention and arrest and reversal of early noncavitated lesions. The decision not to treat, or to prevent, arrest, reverse, and/or surgically treat, are choices based upon these factors. Risk indicators also are considered in estimating future disease. Thus, diagnostic techniques and the influence of risk indicators need to be evaluated for all teeth surfaces and patients of all ages.