Pediatric mandibular fractures are not commonly encountered. The elasticity of bones in a child prevents loss of continuity of bone and rather results in a bending of a cortex termed as a greenstick fracture. Occlusion is rarely a problem as there is no disruption or mild changes are remodeled during the development of permanent dentition. In case of a severely displaced fracture the treatment option can vary from intermaxillary fixation, cap splints to plating with mini plates or resorbable plates.

Arch bar fixation and wiring
In full deciduous dentition, the arch bar fixation or wiring is difficult due to the morphology of the deciduous teeth as the area of maximum convexity is at the gingival third of the crown resulting in slipping of wires. The roots of the deciduous teeth do not tolerate force needed to tighten the wires . Miniplates needs caution so as not to injure the tooth buds of the permanent teeth and may need to be removed after osteosynthesis in growing children. Resorbable plates, eliminates the need for the second surgical procedure for the removal but the risk of damage to the tooth buds do exist.
As far as the healing of wounds in general is concerned, the jaws and face have one great advantage, and that is their copious blood supply; consequently, in major injuries of the jaws it is possible to be much more conservative with comminuted bone fragments and lacerated soft tissue than it is in other regions of the body. On the other hand, the jaws have one great disadvantage in this respect, and that is the presence of teeth; teeth adjacent to the site of fracture may be the cause of complications if they are fractured themselves, displaced, have their adjacent mucoperiosteum detached, or even if they are intact. It is remarkable to see how much more readily healing and union occur in a grossly comminuted fracture of an edentulous mandible than in a similar fracture where teeth are present.

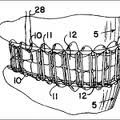
Cap splint and circumandibular wiring. copyright of Springr Images
Cap splints are the good old remedy that comes in handy to manage paediatric fractures. The traditional cap splints made of steel or acrylic are cumbersome to make and will need a technician to make them. They are also very thick and may interfere with occlusion. They also consume lot of time in fitting them on to the teeth to reduce the fracture. On the other hand the thermo forming splints which were initially used as bleaching trays, can be used as Splints. They are available in 1mm, 2mm, 3mm and 4mm thickness and can be trimmed with a pair of scissors or acrylic burs. Thickness of 2mm and above provides adequate immobilization for fracture fragments. The even thickness of the splint also helps in maintaining the occlusion in a reasonable relationship is also provides a increase in joint space and since it is just an intraarch stabilization allows active mouth opening which is a important to avoid any ankylosis of the temperomandibular joint.
Sectional Acrylic Cap Splint:
Synonyms: stout’s or ribbon splint.
Uses:
- Immobilization of dento alveolar structures
- Mandibular fractures.
Advantages:
- Simplicity of the appliance
- Little lab equipment is required for its construction.
 Procedure Of Splinting Using Sectional Acrylic Cap Splint:
Procedure Of Splinting Using Sectional Acrylic Cap Splint:
- It consists of acrylic band or flange.
- Undercuts need not be eliminated.
- By embracing the crown and more especially the interdental spaces excellent retention is obtained.
- 1cm in diameter is situated on the buccal aspect of  splint.
- If displacement is present then obtain a working model, correcting this my dividing the model to wire connectors are adapted.
- From half round1.25 mm diameter of stainless steel wire around the distal aspect and then splint is fabricated in wax.
- Wire ends are left long in order to obtain retention.
- An essential component of this splint is the formation of wax button approximately 1cm in diameter is situated on the buccal aspect of splint.
- The model with wax splint is then invested making sure that the wire inserts are secured in the plaster matrix.
- Following separation of two halves the flask, the wax is  boiled out and the plaster surface painted with cold mould seal.
- If splint is urgently requires then cold cure acrylic is used.
- When processed, splint is removed from plaster, trimmed and polished.
- Splint is sectioned vertically retaining the button, longitudinally along any edentulous spaces.
- Allows splint to be opened out and sprung into position on the model.
- Fixation into the mouth is obtained by passing a soft stainless steel wire around the vertically divided button and through holes drilled horizontally through any edentulous areas.
- This will firmly adapt the splint into all the retaining sites to obtain adequate stability and immobilization.