LINGUAL BAR WITH CONTINUOUS BAR INDIRECT RETAINER
SYNONYMS: KENNEDY BAR, SPLIT LINGUAL BAR, DOUBLE LINGUAL BAR
Indications:
1. Situations where the major connector must contact the natural teeth to provide bracing and indirect retention and there are open cervical embrasures which contraindicate the use of a lingual plate. There must be adequate space for the lingual bar portion of the major connector.
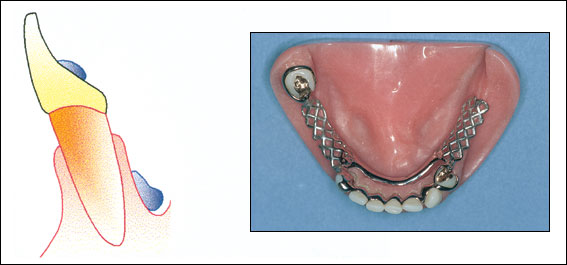
Kennedy Bar
Contraindications:
1. Where a lingual bar or lingual plate will suffice.
2. Any contraindication for a lingual bar.
3. Any contraindication for a lingual plate except open cervical embrasures.
4. Diastemas.
Advantages:
1. More rigid than lingual bar.
2. Covers less tooth and tissue surface than lingual plate.
Disadvantages:
1. Very complex design.
2. May be objectionable to patient because there are four edges exposed to the tip of the tongue.
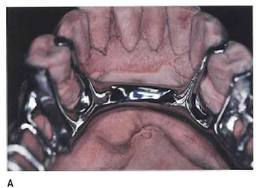
LABIAL BAR (OR PLATE)
Indications:

Lingual tori
1. Lingually inclined teeth preventing the use of a lingual mandibular major connector.
2. Lingual tori or exostoses which cannot be removed surgically, avoided in the removable partial denture (RPD) design, or covered by the framework with adequate relief.
3. A lingual major connector cannot be used because of the slope or undercut of the lingual alveolus.
4. The patient cannot tolerate a lingual major connector.
5. Diastemas and open cervical embrasures contraindicating a lingual plate.
Contraindications:
1. A lingual major connector may be used.
2. Facial tori or exostoses.
3. The facial alveolar ridge is undercut.
4. High facial muscle attachments which would result in less than 3 mm of space between the superior edge of the labial bar and the marginal gingiva of the teeth.
Advantages:
1. Can be used where lingual major connector cannot
Disadvantages:
1. A labial major connector is longer than a lingual major connector and, therefore, must be wider and/or thicker or larger to provide the necessary rigidity.
2. A labial major connector may be visible when the patient smiles and it may distort lip contour resulting in poor esthetics.
3. Difficult to add prosthetic teeth to framework.
CINGULUM BAR
Indications:
Lingual bar with cingulum bar (continuous bar)
1. Height of activated lingual frenum and floor of the mouth at the same level as marginal gingiva.
2. Inoperable tori or exostoses at the same level as the marginal gingiva.
3. Severely undercut lingual alveolus
4. Concern that a major connector traversing the gingival sulcus will cause a periodontal problem.
5. Considerable gingival recession.
Contraindications:
1. When a simpler major connector may be used. Simplification of the design of the denture is always the key to increase patient’s tolerance towards the prosthesis.
2. Diastemas and open cervical embrasures where the metal will show. This will compromise the esthetics and is not appealing to the majority of the population.
Advantages:
1. Can be used where lingual bar and lingual plate cannot.
2. Does not traverse the marginal gingiva or overlay the lingual alveolus.
3. Easy to add prosthetic teeth to framework. This is advantageous if more teeth are to be added to the RPD in the near future.
Disadvantages:
1. Must be bulky to have sufficient rigidity and thus may be objectionable to the patient.
SUBLINGUAL BAR
Indications:
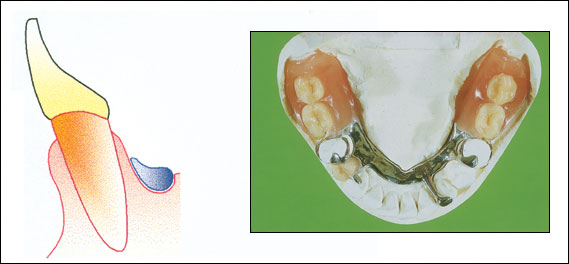
Sublingual bar
1. Bracing and indirect retention can be provided by clasps and indirect retainers and future additions of prosthetic teeth to the framework are not anticipated.
2. Severely undercut lingual alveolar ridges.
3. Distal extension RPD situations with sloped or parallel lingual alveolar ridges where a lingual bar would rotate into the lingual alveolus as the base area rotates tissueward.
4. Diastemas and open cervical embrasures of anterior teeth.
5. Overlapped anterior teeth.
6. Intolerance to other lingual major connectors.
Contraindications:
1. Where a lingual bar or lingual plate will suffice.
2. Situations where bracing and/or indirect retention must be provided by contact of the major connect with the teeth.
3. Situations where future additions of prosthetic teeth to the framework are anticipated.
Advantages:
1. Sublingual bar does not contact anterior teeth or lingual alveolus.
2. More esthetic than other lingual major connectors because of its location.
3. More rigid than lingual bar because bulk of metal is horizontal rather than vertical.
Disadvantages:
1. Requires border molded impression of floor of mouth for accurate placement of major connector.
2. Difficult to add prosthetic teeth to framework.
3. Most patients prefer a lingual plate to a sublingual bar.
The superior edge (1-2 mm) of mandibular major connectors should contact the teeth or tissues to prevent a space which would allow food impaction and accumulation and/or would be noticeable to the patient. The major connector below this contact area should be relieved to prevent contact of the framework with the teeth and/or tissues. The amount of relief depends on the amount of anticipated tissueward movement of the RPD plastic base.
The POLISHED SURFACE (side away from the teeth and tissues) of RPD frameworks is finished smooth with rubber wheels and highly polished.
The TISSUE SURFACE (side next to the teeth and tissues) of mandibular RPD frameworks is finished smooth with rubber wheels and highly polished.